

Do Steroid Injections Help Degenerative Disc Disease? My Pain Management Experience
- Apr 11, 2025
- 9 min read
Updated: May 19

When I walked into pain management for degenerative disc disease, I thought I was entering a room where my pain would finally be explained.
I expected someone to walk me through my imaging, show where my pain might be coming from, and help me compare my options. I wanted to understand the difference between managing symptoms and actually supporting healing. I wanted a doctor to look at my body as a whole system, not just as a painful location that could be injected.
Instead, I left feeling rushed toward a steroid injection before I fully understood what it would do, how long it might last, what risks came with it, or whether it was treating the source of my pain or simply quieting the signal.
I am not against pain management. Pain relief matters. Anyone who has lived with chronic back pain knows that relief is not superficial. It can mean sleeping through the night, walking without fear, showing up for your children, and having enough capacity to participate in physical therapy.
But I also believe patients deserve more than a procedure recommendation. We deserve context. We deserve options. We deserve to understand whether a treatment is meant to help us move toward recovery or simply manage pain in repeating cycles.
That question became especially important to me when steroids entered the conversation.
Do Steroid Injections Help Degenerative Disc Disease?
Steroid injections may help some people with certain types of spine-related pain, especially when inflammation or irritated nerves are involved. Epidural steroid injections place anti-inflammatory medication into the epidural space around spinal nerves, and Cleveland Clinic describes them as a pain-relief option for certain causes of chronic low back pain, particularly herniated discs and spinal stenosis.
But steroid injections do not regenerate discs. They do not reverse degenerative disc disease. Their main purpose is usually to reduce inflammation and provide pain relief.
That distinction matters because “less pain” and “healing” are not always the same thing.
For some people, temporary relief can be meaningful. It may create enough breathing room to move, strengthen, sleep, and return to physical therapy. Cleveland Clinic notes that lumbar epidural steroid injections are often intended to provide enough short-term pain relief for people to begin or continue physical therapy, not to cure back pain.
That is a reasonable goal. But it should be clearly explained.
When I was sitting in that appointment, I did not feel like I was being educated about a temporary tool inside a larger recovery plan. I felt like I was being moved toward the procedure that happened to be available in that office.
What Steroids Can and Can’t Do for Back Pain
Steroids are anti-inflammatory medications. In the context of back pain, they may be used to calm inflammation around irritated nerves or painful structures. Epidural steroid injections can sometimes provide relief for days, weeks, or months, depending on the person and the underlying condition.
What they cannot do is rebuild a damaged disc, restore disc height, correct poor movement patterns, strengthen weak muscles, or address the full complexity of chronic pain.
That does not make them useless. It makes them limited. And limited treatments still deserve honest conversations. I wish the appointment had started with questions like:
Where exactly do we think my pain is coming from? Is this injection diagnostic, therapeutic, or both? What result would tell us the injection worked? What would we do next if it didn’t?
How does this fit into a long-term plan?
Those questions would have made me feel like a participant in my care instead of a passenger in a system I did not fully understand.
My First Pain Management Appointment
By the time I saw pain management, I had already been living with the emotional weight of my diagnosis. Degenerative disc disease sounds terrifying when you first hear it. Even the name feels cruel. It makes your body sound like it is falling apart in slow motion. I was scared, but I was also motivated.
I wanted to learn. I wanted to make smart decisions. I wanted to protect my future body, not just numb my present pain. That's why the appointment disappointed me so much.
The conversation seemed to move quickly toward a steroid injection. I did not feel like enough time was spent reviewing my imaging in detail, explaining the likely pain generators, or helping me understand the full range of options.
From a patient perspective, it felt transactional. I do not say that lightly. I know doctors are busy. I know pain management practices see patients all day long. I know steroid injections can be appropriate for some people. But when you are the person sitting on the exam table, trying to make sense of a life-altering diagnosis, efficiency can feel like dismissal.
I needed someone to slow down. I needed someone to tell me not only what they could do, but why they believed it was the right next step.
Why I Questioned the Recommendation
Pain can make you vulnerable. When you are hurting, you are more likely to say yes to anything that promises relief. That vulnerability should be handled carefully. A patient in pain deserves more explanation, not less.
I wanted to know whether the injection was being used to identify the source of my pain, reduce inflammation, or temporarily calm symptoms. I wanted to understand whether my pain was thought to be disc-related, nerve-related, SI joint-related, facet-related, muscular, or some combination of all of the above.
Instead, I felt like I was being offered a single pathway before the whole map had been shown to me.
That experience pushed me to research more on my own.
What the Research Says About Epidural Steroid Injections
The research on epidural steroid injections is mixed, and the benefits depend heavily on the condition being treated. A 2025 American Academy of Neurology systematic review found that epidural steroid injections may have limited effectiveness. The review found they may modestly reduce pain in some situations for up to three months and reduce disability for some people for six months or more. The review focused on radiculopathy, which involves a pinched nerve, and spinal stenosis, where the space around the spinal cord or nerves becomes compressed.
That matters because “back pain” is not one single thing.
Pain from an irritated nerve may respond differently than pain from disc degeneration alone. Sciatica-like symptoms may require a different conversation than axial low back pain. A treatment that makes sense for one pain pattern may not be the right tool for another.
This is why I believe the diagnosis conversation matters so much. Patients should understand what problem the procedure is meant to solve.
Why Doctors Use Steroid Injections Diagnostically
One part of steroid injections that I wish had been explained more clearly is their diagnostic use.
Sometimes injections are not only about relief. They may also help identify where pain is coming from. If a targeted injection reduces pain, that response can give the doctor information about the likely source.
That is valuable.
But from the patient side, it should be made explicit. There is a difference between:
“We think this will reduce your pain,” and “We are using this injection to help confirm whether this structure is contributing to your pain.”
Those are different conversations. They lead to different expectations.
If the injection is diagnostic, tell me what we are testing. If it is therapeutic, tell me how long relief typically lasts. If it is both, explain how we will interpret the results.
Patients can handle nuance. In fact, many of us are desperate for it.
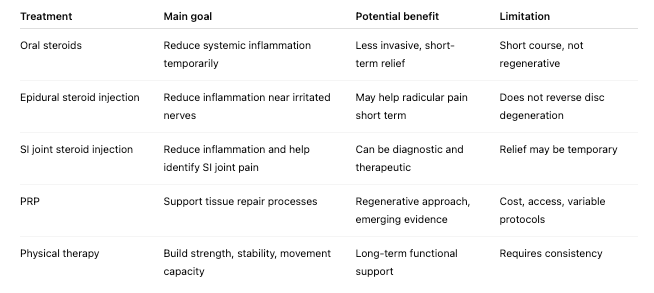
Steroid Injections vs. PRP vs. Physical Therapy: What Each Treatment Is Trying to Do
Why I Started Looking Into PRP
After that appointment, I became more interested in regenerative medicine, especially platelet-rich plasma, or PRP. PRP appealed to me because it was presented as a treatment that might support the body’s repair processes rather than only quieting inflammation.
I did not just want to mute pain. I wanted to understand whether there were options that could support tissue health, function, and long-term improvement.
That said, PRP is not magic. The research is still evolving, protocols vary, and access can be difficult because many patients pay out of pocket. A 2023 systematic review on platelet-rich plasma for low back pain described PRP as generally effective and safe for degenerative low back pain, while also making clear that this is an area where evidence and treatment approaches continue to develop.
For me, PRP represented a different kind of question.
Instead of asking only, “How do we reduce pain right now?” I started asking, “What supports the body’s ability to heal, stabilize, and function better over time?”
That question changed the way I approached my care.
Steroid Injections vs. PRP: Pain Relief vs. Regeneration
The simplest way I came to understand the difference is this: Steroid injections are generally anti-inflammatory. PRP is generally considered regenerative or orthobiologic.
That does not automatically make PRP better. It means the intention is different.
Steroids may be useful when inflammation is driving pain and a person needs relief to function. PRP may be considered when the goal is to support a healing response in damaged or irritated tissue. Both should be discussed with appropriate medical nuance. The problem is that many patients are never offered that broader conversation.
Instead, patients are often presented with the tools available inside a particular practice, not necessarily the full landscape of options. That is why patient advocacy matters so much. Sometimes the treatment you are offered first is simply the treatment the office performs most often.
That does not mean the recommendation is wrong.
But it does mean you are allowed to ask what else exists.

Questions I Wish I Asked Before a Steroid Injection
If I could go back to that first pain management appointment, I would ask more direct questions.
Here are the ones I would bring now:
What exact structure do you believe is causing my pain?
Is this injection diagnostic, therapeutic, or both?
Are you treating disc pain, nerve pain, SI joint pain, facet pain, or inflammation?
What result would tell us this injection worked?
How long does relief usually last for someone with my diagnosis?
What happens if it does not work?
How many injections would you recommend in a year?
What are the risks for my specific body and medical history?
Will this help me participate more fully in physical therapy?
Are there less invasive options to try first?
What are the alternatives, including PRP, physical therapy, medication, or lifestyle changes?
If PRP is not offered here, is that because it is inappropriate for me or because this practice does not provide it?
That last question is important. Sometimes a treatment is not mentioned because it is not right for you. Other times, it is not mentioned because it is not part of that clinic’s business model. Patients deserve to know the difference.
Pain Relief Is Not the Same as a Long-Term Plan
One of the biggest lessons I learned is that pain relief and healing can overlap, but they are not identical. Pain relief can be necessary. There is no nobility in suffering when relief is available and appropriate. But if a treatment only lowers pain temporarily without helping you build strength, improve function, address contributing factors, or understand your body better, then it may not be a complete plan.
For me, the most useful care has been care that helps me connect the dots.
Physical therapy helped me understand weakness, movement patterns, breath, glute strength, and core stability. Research helped me understand the difference between anti-inflammatory and regenerative approaches. My own lived experience helped me recognize when I felt supported by a provider and when I felt processed.
I no longer want care that simply asks, “Where does it hurt?”
I want care that asks, “Why is this body struggling, and what can we do to support it from more than one angle?”
FAQ: Steroids, PRP, and Degenerative Disc Disease
Do steroid injections help degenerative disc disease?
They may help reduce inflammation and provide temporary pain relief for some people, especially when irritated nerves, radiculopathy, spinal stenosis, or sciatica-like symptoms are involved. They do not reverse disc degeneration or regenerate damaged discs.
How long do steroid injections last for back pain?
Relief varies. Some people experience temporary relief for days, weeks, or months. Cleveland Clinic notes that pain relief from epidural steroid injections may last several days or months, depending on the person and condition.
Are steroid injections regenerative?
No. Steroid injections are anti-inflammatory. They may reduce pain and swelling, but they are not designed to regenerate discs or rebuild tissue.
Are steroid injections better than PRP?
They are different tools. Steroids are generally used to reduce inflammation and pain. PRP is considered a regenerative treatment, but research is still evolving, protocols vary, and it may not be covered by insurance.
Are epidural steroid injections risky?
They are commonly performed, and many people tolerate them well, but they are not risk-free. Potential complications can include infection, headache, nerve injury, numbness, weakness, or other serious events in rare cases. Patients should ask their provider to explain their specific risks and alternatives.
What should I ask before getting a steroid injection?
Ask what structure is being treated, whether the injection is diagnostic or therapeutic, how long relief may last, what risks apply to you, what alternatives exist, and how the injection fits into your long-term care plan.
Final Thoughts: I Wanted More Than a Procedure
That appointment taught me to stay awake inside my own care. Not suspicious of every recommendation, and not closed off to medical treatment, but alert to the difference between temporary relief and a long-term plan. A procedure can be useful and still incomplete. Patients in pain deserve care that respects how vulnerable they are when they are scared, exhausted, and desperate for relief.
Degenerative disc disease made me afraid of my body at first.
But the harder part was realizing how much I would have to advocate for it.
That advocacy has become part of my healing.
My spine is not just a site of pain. It's part of my life, my movement, my motherhood, my future, and my ability to keep becoming myself.
I want care that honors that whole picture.

